
In surgical treatment for cancer, the tissue surrounding the tumor is typically also removed. This edge or boundary is then examined by a pathologist to determine if there are any cancer cells present. Achieving a ‘clear margin’ is a critical goal because it greatly influences the likelihood of the cancer returning or recurring in the same area.
About 50% of patients with colorectal cancer develop metastases to the liver during their illness. The main treatment aim for these patients is to remove the tumor completely with clear margins of at least 1 mm, called ‘R0 resection’, to improve survival rates and limit the spread of the cancer.
Enhancing Tumor Visibility Using ICG
The increasing adoption of minimally invasive techniques like laparoscopic and robot-assisted liver surgery over the last decade has been shown to reduce hospital stays and complications while maintaining oncologic outcomes. However, these techniques can make tumor identification and margin assessment more challenging.
To overcome this, a study by the Dutch Liver Surgery Group led by Rutger-Jan Swijnenburg implemented fluorescence-guided minimally invasive liver surgery across nine Dutch liver centers. The study was set up in close cooperation with Alexander Vahrmeijer at Leiden University Medical Center, an expert in fluorescence-guided surgery.
This innovative imaging technique uses Indocyanine Green (ICG), a medical dye, to enhance the visibility of cancerous tissues during surgery. ICG absorbs light and emits fluorescence in the near-infrared spectrum, which penetrates several millimeters into tissue. This enhances tumor visibility without being visible or harmful to the human eye. A specialized camera captures the fluorescent signal during surgery and displays it on a monitor to guide the complete removal of tumor tissues while sparing as much healthy tissue as possible.
With the use of fluorescence, we have now further improved minimally invasive surgeries by simply being able to visualize the tumors better. We can now predict during surgery with higher confidence whether the metastasis is being removed in its entirety, and possibly remove
additional tissue if the margins are tight."

Rutger-Jan Swijnenburg, Principal Investigator and Oncological Surgeon
at Cancer Center Amsterdam.
Highlighting the Margin
The recent MIMIC (Minimally Invasive, Indocyanine-Guided Metastasectomy in Patients With Colorectal Liver Metastases) trial investigated whether ICG could improve the diagnostic accuracy of real-time tumor margin assessment and RO resection rates.
Patients involved in the study received an injection of indocyanine green (ICG) one day prior to their liver surgery. Normally, liver cells metabolize ICG and excrete it through the bile ducts. However, liver cells adjacent to a tumor often have impaired function and do not process ICG effectively—a condition known as 'cholestasis.' This results in a distinct fluorescent ring approximately 8mm wide around the tumor. During the surgery, this ring is completely removed along with an additional margin of healthy liver tissue.
Elucidating Real Time Surgery
The absence of fluorescence from the area following removal predicted a successful RO resection in 92.4% of the cases, a significant increase compared to traditional surgery.
The technique also allowed surgeons to modify the surgical plans based on real-time feedback. In more than one-quarter of the procedures, surgeons altered their approach due to the insights provided by the imaging. Moreover, the researchers also found that the use of ICG fluorescence resulted in the resection of additional tissue in a substantial number (8.5%) of patients. This adaptability contributed significantly to the increased RO resection rate.
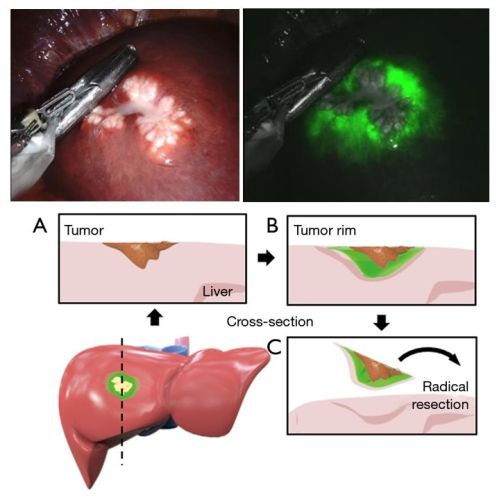
Photos of a liver metastasis with fluorescent margin and schematic overview of resection.
Illuminating the Path Ahead
In this study, surgeons at the participating hospitals were trained to use fluorescence-guided surgery to ensure the complete removal of metastases. Despite an initial learning curve, the study authors indicated that the adoption of fluorescence-guided surgery can be expanded beyond specialized centers by training surgical personnel and providing preset imaging protocols. Cameras used during keyhole surgery or robotic surgery can easily be equipped with the technology to detect fluorescence.
By integrating ICG-fluorescence imaging into surgical practices, there is a potential to significantly enhance the precision of tumor resections, ultimately improving the prognoses for patients.
Future studies are expected to further validate the patients’ benefits and examine the cost-effectiveness of fluorescence-guided surgery through a randomized controlled trial format.
For more information, contact Rutger-Jan Swijnenburg, or read the publication:
Achterberg F.B., Bijlstra O.D., Slooter M.D., et al. ICG-Fluorescence Imaging for Margin Assessment During Minimally Invasive Colorectal Liver Metastasis Resection. JAMA Netw Open. 2024;7(4):e246548. doi:10.1001/jamanetworkopen.2024.6548
Participating hospitals
Amsterdam UMC – Cancer Center Amsterdam, OLVG (both Amsterdam), Jeroen Bosch hospital (Den Bosch), Leidsch University Medical Center (Leiden), UMC Utrecht, st. Antonius hospital (both Utrecht), Medisch spectrum Twente (Enschede), UMC Maastricht, Amphia hospital (Breda)
Involved researchers affiliated with Amsterdam UMC / Cancer Center Amsterdam
Friso B. Achterberg
Okker D. Bijlstra
Maxime D. Slooter
Mark C. Boonstra
Babs M. Zonderhuis
Rutger-Jan Swijnenburg
Funding
This study was funded by the Dutch Cancer Society (KWF).

Related articles
Improved precision using robotics for cancer surgery
Text by Laura Roy.
This article was created for Cancer Center Amsterdam.
Follow Cancer Center Amsterdam on LinkedIn & X/ Twitter.
© 2024 New Haven Biosciences Consulting– All rights reserved.