
Exercise and the heart
Endurance exercise is known to cause temporary changes in the heart, including short‑term elevations in cardiac biomarkers and subtle alterations in cardiac function. Individual studies have reported post‑marathon changes in small cohorts, but results have often been inconsistent and difficult to compare. “We know that endurance exercise challenges the heart, but we still do not fully understand whether the immediate response is purely benign or a signal of something that might become problematic over time,” says principal investigator Harald Jørstad.
What this study adds
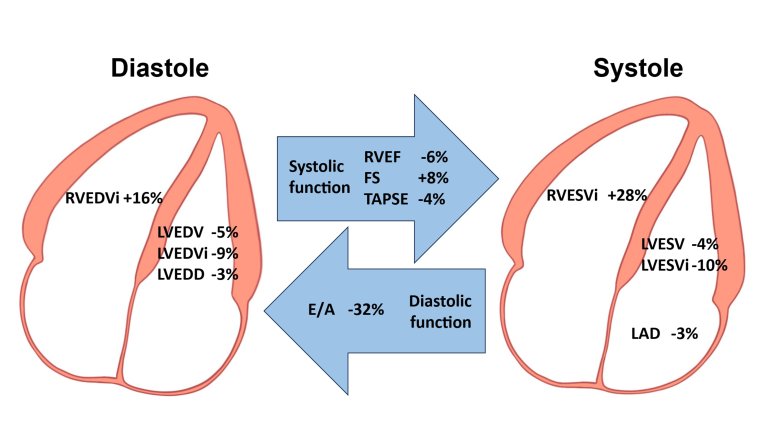
In the study, the researchers examined runners before and after a marathon and measured both blood biomarkers and cardiac structure and function. They found that circulating levels of cardiac troponin T (cTnT), cardiac troponin I (cTnI) and NT‑proBNP increase after marathon running. Also, chamber volumes and cardiac function are moderately altered after completing a marathon.
These responses vary with age, sex, training status and marathon performance, indicating substantial inter‑individual variability. “Our data suggest that a one‑size‑fits‑all interpretation of post‑marathon test results is not appropriate,” explains PhD candidate Inarota Laily. “Two runners may show very different biomarker patterns after running the same race, depending on their background and training.”
Normal response or early warning?
A central question in sports cardiology is whether these acute changes are part of a normal physiological response to endurance exercise, or whether they may represent early markers of adverse cardiac remodeling in a subset of athletes. The team emphasizes that, based on current evidence, the observed changes after marathon running are most likely physiological in recreational and trained runners without known heart disease. However, they also highlight important knowledge gaps. “For most healthy runners, these biomarker rises probably reflect how the heart copes with a major endurance challenge,” notes Jørstad. “At the same time, we cannot yet exclude that in some individuals, repeated episodes might contribute to subtle, long‑term changes in cardiac structure or function.” “This ambiguity is exactly why we need better data,” adds Laily. “Our study is a step forward, but it also shows how much more we need to learn before we can fully reassure every athlete or tailor advice to those at higher risk.”
Implications for research
The study calls for a more standardized and nuanced approach in future research on exercise‑induced cardiac changes. According to the authors, three aspects deserve particular attention. Firstly sex‑stratified analyses are needed to understand differences between male and female athletes. Secondly, standardized biomarker sampling is necessary, including timing and methodology, to improve comparability between studies. Lastly, comprehensive reporting of training status, race performance, and baseline fitness, are needed to better capture inter‑individual variability. “If we want robust conclusions, we have to move beyond small, heterogeneous datasets,” says Harald Jørstad. “Standardising how we collect and report data is crucial for the field.”
Towards long‑term answers
The researchers underline that longitudinal follow‑up is essential to determine whether repeated acute changes after endurance events translate into long‑term cardiac adaptations. “Cross‑sectional snapshots only tell us what happens around one race,” explains Laily. “What we truly need are long‑term studies following runners over years, linking their training and race histories to detailed cardiac assessments.” “Ultimately, our goal is to give athletes, clinicians and policymakers evidence‑based guidance,” concludes Jørstad . “That means identifying who can safely push their limits, and who might need closer monitoring or a different training strategy.
These findings were published in the BMJ Open Sports and Exercise Medicine. The project was funded by the Indonesia Endowment Fund for Education.